| PSY 448 Clinical Neuropsychology |
Updated:August 31, 2025 |
|
| PSY 448 Clinical Neuropsychology |
Updated:August 31, 2025 |
|
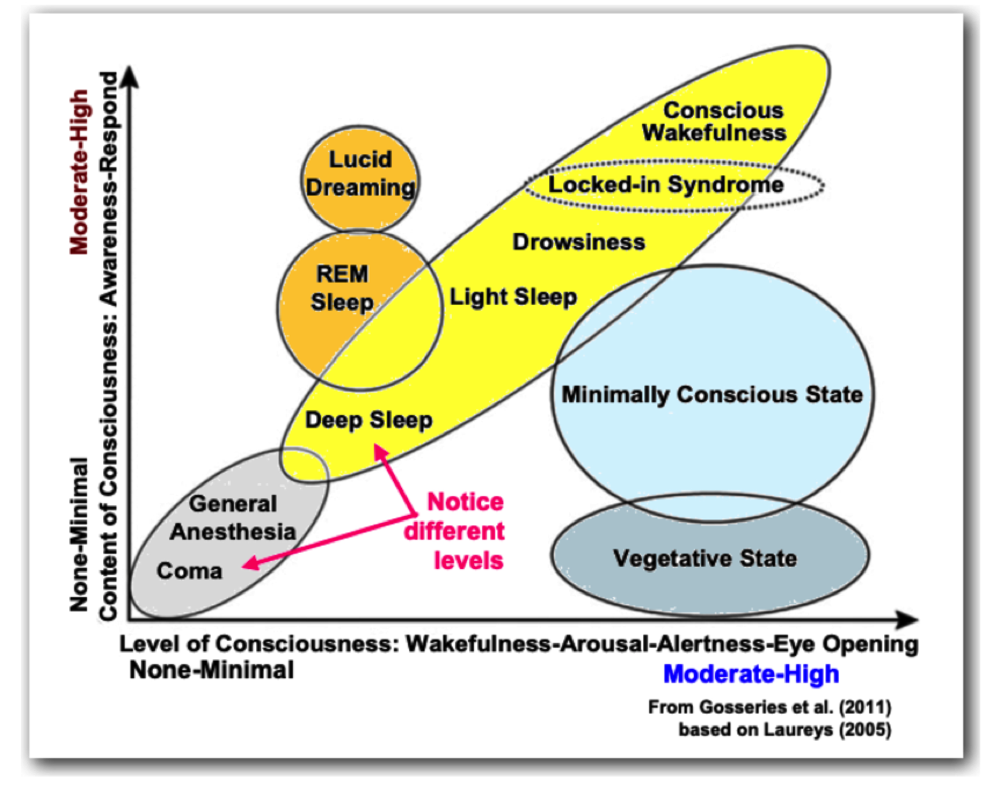
A. The Range of Consciousness
Consciousness in neurology and neuroscience is understood to have two different components:
1. Arousal (i.e., the level of consciousness): How aroused, alert, awake a person is?
2. Awareness (i.e., the content of consciousness): Is the person aware of what is around them and can respond?
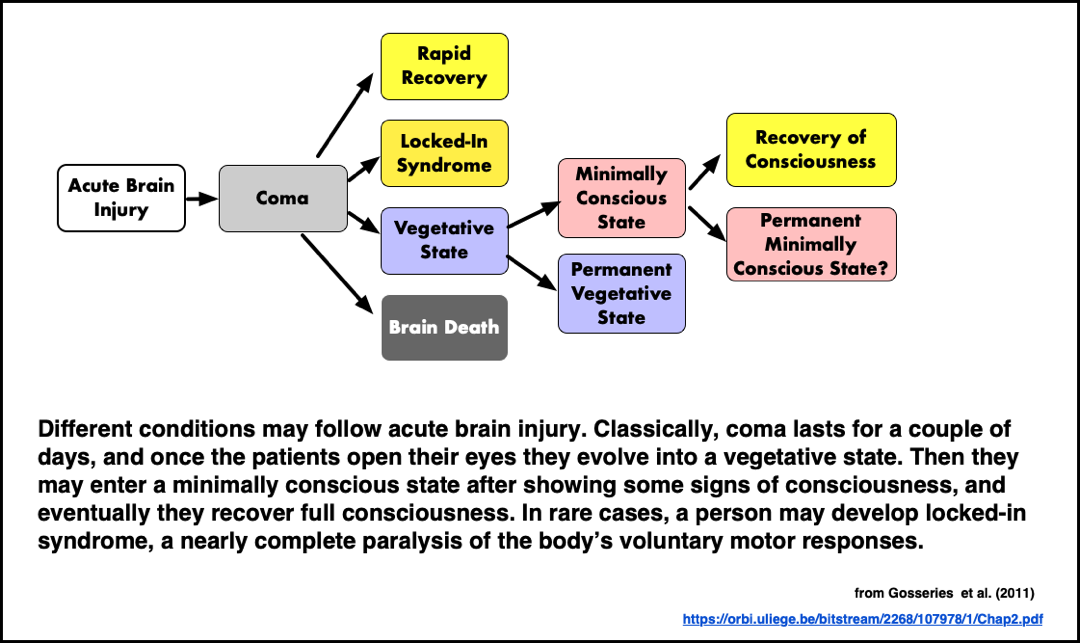
B. Disorders of Consciousness
What kinds of disorders of consciousness arise if an individual has suffered an acute brain injury?
1. Coma: unconsciousness due to head trauma, disease, or stroke in which an individual cannot be awakened or brought to consciousness
2. Vegetative State (Unresponsive Wakefulness Syndrome): alternation between sleep and moderate arousal without awareness of surroundings. No clear sign of purposeful activity though there may be some cognitive activity. Some individuals do not progress beyond this state.
3. Minimally Conscious State: Brief periods of purposeful activity and some speech comprehension (but no speech production).
- Cognitive Motor Dissociation. In a landmark international study, Bodien et al. (2024) studied 353 adults with significant impairment of consciousness scanning their brains using either fMRI or EEG. As described by Nowogrodzki (2024) “During each scan, people were told to imagine themselves playing tennis or opening and closing their hand. The commands were repeated continuously for 15– 30 seconds, then there was a pause; the exercise was then repeated for six to eight command sessions. Of the physically unresponsive people, about 25% showed brain activity across the entire exam for either EEG or fMRI. The medical name for being able to respond mentally but not physically is cognitive motor dissociation.” (emphasis added) This study expanded earlier findings from 2019 by other researchers that some individuals with Unresponsive Wakefulness Syndrome might actually be aware of what is happening around them.
4. Locked-In Syndrome: Locked-in syndrome is a rare disorder of the nervous system. People with locked-in syndrome are:
- Paralyzed except for the muscles that control eye movement
- Conscious (aware) and can think and reason, but cannot move or speak; although they may be able to communicate with blinking eye movements
5. Brain Death
- No sign of brain activity and no response to stimuli (for 24 hours). These criteria include (1) a total unawareness to externally applied stimuli, (2) no movements or breathing, (3) no reflexes [e.g., pupils fixed and dilated], and a flat EEG. The tests for 1 through 4 must be repeated 24 hours later with no change.
- Originally proposed by the Ad Hoc Committee of the Harvard Medical School to Examine the Definition Brain Death in 1968.
- A model state law, the Uniform Determination of Death Act (UDDA), was proposed in 1981 as a result of deliberations among multiple professional groups (e.g. the AMA, ABA, etc.) to implement the Harvard Medical School guidelines. Currently 37 states, DC, and the US Virgin Islands have enacted this law as the legal standard to determine brain death.
- The brain cannot itself sustain the body without significant life support. "The term brain death is defined as "irreversible unconsciousness with complete loss of brain function," including the brain stem, although the heartbeat may continue." (Encyclopedia of Death & Dying). In the UDDA, the standard is stated in this fashion: "An individual who has sustained either (1) irreversible cessation of circulatory and respiratory functions, or (2) irreversible cessation of all functions of the entire brain, including the brain stem, is dead."
- Note, though, that there has been continuing controversy over these criteria. One of the contributing factors is that the healthy organs of brain dead individuals can be transplanted into those who are critically in need of such transplants. There is a risk that the incentive to "harvest" organs might undermine the full determination of brain death required by the law. Indeed, there was a case in Kentucky in October 2024 where just such a possible tragic error was reported as averted (see https://www.npr.org/sections/shots-health-news/2024/10/16/nx-s1-5113976/organ-transplantion-mistake-brain-dead-surgery-still-alive).
- Greer et al. (2025) noted below offers very recent overview of the whole topic of brain death. And, it is available to LMC students from computers on the college's internet.
References
Bobien, Y. G., Allanson,J., Cardone, P.,… and Schiff, N.D. (2024) Cognitive motor dissociation in disorders of consciousness. New England Journal of Medicine, 391, 598-608. https://dx.doi.org/10.1056/NEJMoa2400645
Greer, D. M., Lewis, A., & Kirschen, M. P. (2025). The neurologist’s imperative in brain death. JAMA Neurology, 82(8), 759-760. https://dx.doi.org/jamaneurol.2025.0191
Nowogrodzki, J. (2024, August 14). One-quarter of unresponsive people with brain injuries are conscious. Nature. https://doi.org/10.1038/d41586-024-02614-z