Forgetting: When Memory Lapses
![[Hermann Ebbinghaus]](../psy101graphics/ebbinghaus.png) A. How Quickly We Forget:
Ebbinghaus's Forgetting Curve
A. How Quickly We Forget:
Ebbinghaus's Forgetting Curve
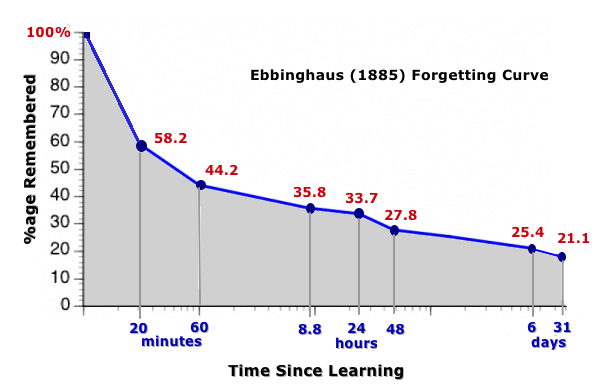
- Earliest
studies of forgetting were done by Hermann
Ebbinghaus (1885)
- Used
trigrams = "nonsense" syllables
(consonant-vowel-consonant, e.g., XOR, LIM, WEP,
etc.).
B.
Measures of Forgetting
- Retention = Proportion of
material which is retained or remembered
- Recall: Reproduce information
without any cues
VS
- Recognition: Select
previously learned information from an array of
options
- Relearning: How long does it
take to relearn what you had previously learned?
C. Why We Forget
1. Ineffective Coding
2.
Decay = memory traces fade with age. Not
true except with dementia.
3.
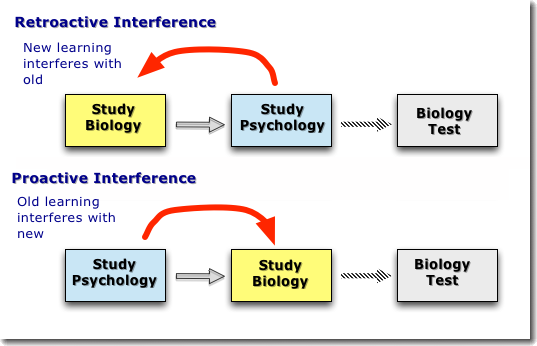
Interference Problem = forgetting
information because of competition from other material
- Retroactive
Interference: New learning interferes with
old learning (NIO)
- Proactive
Interference: Old learning interferes with
new learning (OIN)
4. Retrieval Failure
5. "Motivated" Forgetting
- Sigmund
Freud (1901): Described a process he called "repression"
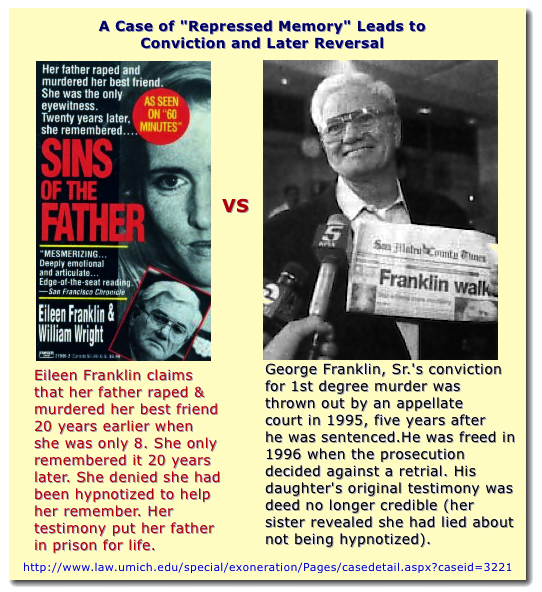 The Repressed Memory
Controversy
The Repressed Memory
Controversy
- 1980s-1990s:
Individuals began reporting to their
therapists the recollection of memories, long buried
from the past, which claimed experiences of sexual
abuse, traumas, and even the witnessing of murder. These
memories were considered to be "repressed" as Freud
suggested.

- Elizabeth
Loftus: research showing some false memories can
be implanted
- Estimate
in experimental studies is 30% of subjects will
develop a false memory and 23% accepted that they had
an experience even though they didn't remember it.
- a
memory report can look like a genuine memory to
observers, even if the person does not explicitly
report remembering the events
- PTSD
patients show too many memories
- Bottom
line
- Abuse
is more widespread than we used to think decades
ago.
- "Repressed
memories" are forms of "believed-in imaginings," that
is, even if not factually true, the person reporting
them believes them to be true and are not deliberately
lying
- Therapists
and others (e.g., police) need to be very careful not
to suggest that there are buried memories
The Physiology of Memory
Neuropsychologists
and neurologists have seen for years that there seem
to be at least two different kinds of amnesia, that
is, an inability to remember what happened in the
past, depending upon when some event like a brain
injury took place.
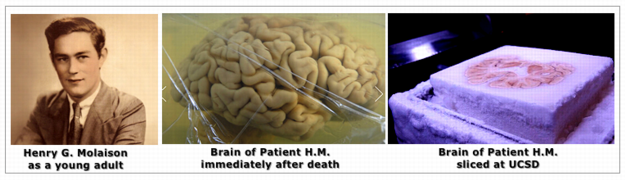
Patient H.M. (Henry Gustav Molaison, 1926-2008)
Here's his story
in a YouTube video [5'25"] from an animated TedEd
presentation.
- Short-term
working memory was fine. He could remember things for 5
to 10 minutes.
- He
could not remember any experience longer than about 5 to
10 minutes, that is, anything that would be a new
addition to his long-term memory. For example, he saw
the same doctors and psychologist day after day, but
never learned who they were.
- He
also had very significant memory loss of events in his
life from before his operation.
- His
overall intelligence remained intact and he could
generally care for himself, carry on conversations, and
enjoy himself with puzzles and other games.
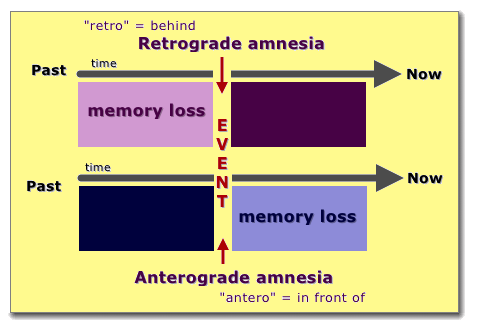
Massive anterograde amnesia = no memory
for any new experiences/learning after operation
Significant retrograde amnesia = very weak memory
for events/experiences from before the operation
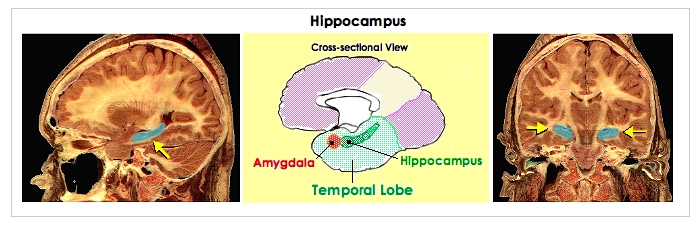
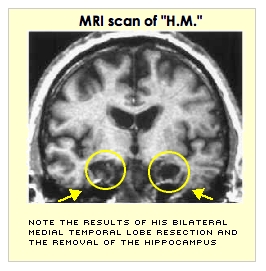
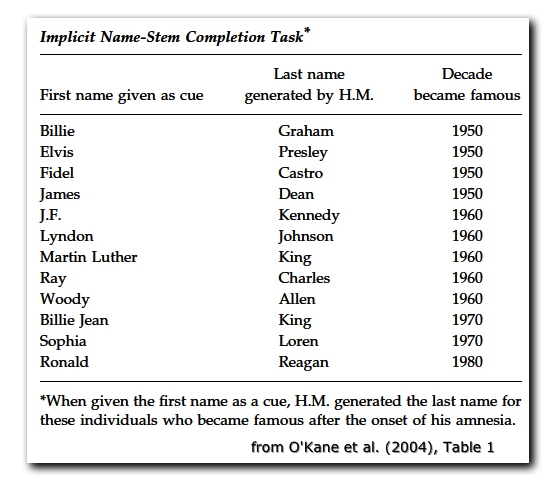
Hippocampus is central to
learning any new explicit or declaratory memory,
but not for implicit or procedural memories (e.g.,
how to do something)